

By Cherob Pacheco, Jiea Sian, and Gabriel Gony Revilla
Introduction
On the 31st of December 2019, Wuhan Municipal Health Commission, China, reported a cluster of pneumonia cases in Hubei Province, which eventually led to the identification of a new coronavirus (2019-nCoV). It took only less than two weeks for the virus to set foot on China’s neighboring countries, with Thailand being the pioneer country outside of China to record a case. With the acceleration of globally reported cases, alarming severity and frightening inactions of respective leaders, the World Health Organization, upon thorough assessment, characterized 2019-nCoV crisis as a pandemic on March 11, 2020. Over 200 affected countries are left to deal with the enduring threats brought about by the crisis. Economic recession, collapsed healthcare system, insufficient government funds, and stagnant movement of life are just some of the aftermaths being experienced by these countries due to COVID-19.
According to the Department of Health (DOH), the Philippines confirmed its first case of the novel coronavirus (2019-nCoV) last January 30, 2020. Thereafter, the country has been grappling with the effects of 2019-nCoV for months now, with communities facing rising infections. In a series of reports published by the DOH, currently at the national level, the Philippines remains in Stage 2, localized community transmission with some geographic areas showing higher transmission intensity and indications of widespread community transmission. And at national level, the bed occupancy rate for COVID-19 allocated beds is currently at 33% occupancy, with variation between regions. Additional beds are being allocated for 2019-nCoV cases, as per the direction of the government. In the past weeks there seem to have been a decrease in daily reported cases, deaths and recoveries by as much as 25%. Additional data validation and harmonization efforts are ongoing. The government is responding across sectors, including through enhanced community engagement, targeted isolation and quarantine measures, expansion of contact tracing and continuous increase in laboratory capacity.
Developed countries are working to replenish shortage of supplies and equipment such as personal protective equipment (PPE) as they are already running low for their local healthcare providers. If first world countries are struggling with their stocks, third world countries are facing even greater struggle. Vaccines are also being developed by these countries with a hope for this pandemic to come to an end. For the time being, like any other country whose health system has been put to the test, the Philippines, with its relatively ill-equipped health system, was expected to be overwhelmed with the surge of COVID-19 cases. A shortage of hospital beds in regular as well intensive care, mechanical ventilators and masks are among the most pressing issues in an archipelago country of 100 million people. Hospitals and health care centers saw the exact opposite where spaces were filled to the brim, patients coming in faster than others could leave. Scenes of cramped hallways and stadiums turned into makeshift hospitals flooded screens for days too many to count.
At present, frontline healthcare workers in the Philippines are badly struggling within a strained healthcare system as they battle both rising COVID-19 infections, and other social concerns such as lack of proper salary compensation, understaffing, and discrimination. The COVID-19 virus, as well as its challenges to healthcare frontline workers, serve as an obstacle the Philippines must address to give better conditions for these frontliners. Several laws such as the Labor Code of the Philippines and Republic Act 7305: Magna Carta of Public Health Workers can be used to address these concerns.
The COVID-19 outbreak in the Philippines shed light on the realities faced by our unsung heroes, our Filipino nurses. For many years, Filipino nurses had been leaving the country in quest for a better life. After failed attempts of fighting for higher wages and better working conditions, they have found refuge in countries which provided them with better opportunities such as to attain financial independence. According to the Department of Labor and Employment (DOLE), an entry-level registered nurse receives an average salary of P8,000 ($158.54) to P13,500 ($267.54) per month. Registered nurses hired by hospitals commonly receive an average salary of P9,757 ($193.36) a month. In government, the average salary per month is around P13,500 ($267.54) while in the private sector, the rate average is around P10,000 ($198.18) per month. On the other hand, according to the 2017 data of the Organization for Economic Co-operation and Development (OECD), Western countries can pay nurses as much as P5 million per year. That’s a dozen times more than the starting annual wage of nurses in the Philippines.
| Average Annual Salary of Filipino Nurses | ||
| Position | Salary Grade | Amount (in thousands) |
| Nursing Attendant I | 4 | P165 684 |
| Nursing Attendant II | 6 | 186 288 |
| Nurse I | 11 | 267 792 |
| Nurse II | 15 | 384 636 |
| Nurse III | 17 | 461 568 |
| Nurse IV | 19 | 561 492 |
| Nurse V | 20 | 632 436 |
| Nurse VI | 22 | 802 404 |
| Nurse VII | 24 | 1 020 888 |
| Nursing School Principal I | 21 | 712 236 |
| Nursing School Principal II | 22 | 802 404 |
| Nursing School Principal III | 23 | 904 308 |
| Ward Assistant | 7 | 197 496 |
| Country | Ave. Annual Salary (in $) | Ave. Annual Salary (in P) | |
| 1 | United States | 75,770 | 3,823,354 |
| 2 | United Kingdom | 45,186 | 2,280,090 |
| 3 | Turkey | 17,445 | 880,279 |
| 4 | Switzerland | 76,162 | 3,843,111 |
| 5 | Spain | 40,656 | 2,051,485 |
| 6 | Slovenia | 26,131 | 1,318,594 |
| 7 | Slovak Republic | 14,942 | 753,948 |
| 8 | Norway | 66,647 | 3,363,009 |
| 9 | New Zealand | 56,318 | 2,841,792 |
| 10 | Netherlands | 61,866 | 3,121,755 |
| 11 | Mexico | 15,235 | 768,765 |
| 12 | Luxembourg | 105,749 | 5,336,082 |
| 13 | Italy | 34,518 | 1,741,769 |
| 14 | Israel | 63,541 | 3,206,259 |
| 15 | Ireland | 57,663 | 2,909,692 |
| 16 | Iceland | 87,639 | 4,422,256 |
| 17 | Hungary | 12,794 | 645,566 |
| 18 | Finland | 42,615 | 2,150,329 |
| 19 | Estonia | 17,417 | 878,872 |
| 20 | Czech Republic | 17,624 | 889,323 |
| 21 | Chile | 34,276 | 1,729,546 |
| 22 | Canada | 54,971 | 2,773,841 |
The severe lack of medical workers threatens the country’s campaign to curb the transmission of the coronavirus disease 2019 (Covid-19) and has compelled hospitals and medical facilities to operate understaffed COVID wards and intensive care units (ICUs). At any rate, the problem of shortage of Filipino nurses in hospitals leading to understaffing has long been a dilemma experienced by the profession. It was only through this pandemic that this problem of shortage has been highlighted as public health workers cry for a timeout. According to the Philippine Nurses’ Association, the nurse-to-patient ratio in government institutions is 1:60, some distance away from the DOH’s ideal ratio of 1:12. With the facts stated, Filipino nurses have to exert more effort of at least five times what is ideal. The phrase “overworked and underpaid” has then become synonymous to the nursing profession.
Filipinos nurses are one of the few professions that are respected in the Philippines (Ordonez, Gandeza, 2004). However, aside from pouring their efforts in fighting the COVID-19, Filipino health workers are yet to fight another enemy: discrimination. In these chaotic times, the culture of fear from contamination is born. There were various instances reported depicting the discrimination faced by medical workers throughout the outbreak of the pandemic. For instance, a community signed a petition banning a nurse from coming home to his barangay for fear that he might be a carrier of the virus. On another note, a nurse was splattered by chlorine by a riding-in-tandem on his way to work. A combination of verbal and physical abuse were faced by the nurses. In spite of the discrimination, Filipino nurses, however, continue to deliver passionate service of caring for people especially in these times of outbreak and setting that are fragile or in conflict.
Objectives
1. To evaluate the enforcement of occupational safety and health laws, regulations, and standards to promote safe and healthful working conditions in the establishments and workplaces of our Philippine nurses.
2. To assess whether or not our nurses are being compensated properly and given the proper working environment in accordance with the provisions of the Labor Code and Republic Act 7305: Magna Carta of Public Health Workers.
Methodology
Research Design
A research design is a plan that guides the investigator in the process of collecting, analyzing and interpreting observations. It is a logical model of proof that allows the researcher to draw inferences concerning causal relations among the variables under investigation (Taole, 2008). A descriptive research design was selected to determine the working conditions of Filipino nurses who are employed in the Philippines based on three aspects: salary, workload and discrimination. A descriptive research aims to accurately and systematically describe a population, situation or phenomenon. Descriptive research is an appropriate choice for this research since the researchers aim to describe the characteristics evolving the practice of nursing in the Philippines on certain points.
Research Approach
In research terminology, population can be explained as a comprehensive group of individuals, institutions, objects and so forth having common characteristics that are the interest of a researcher. On the other, a sample is the specific group of individuals that the researchers will collect data from. In this study, the population consists of the Filipino nurses employed in the Philippines, whether in a public or private hospital. The sampling frame comprises the Filipino nurses employed in the hospitals of Negros Occidental and Iloilo. For the purpose of this research, the researchers furnished a questionnaire to be used to gather data from the respondents. The group took advantage of the online feature of sending out questionnaires, and as well as distributed printed questionnaires to hospitals. The questionnaire was chosen as a research instrument since it is a quick, efficient, reliable and timely way of collecting data from the respondents.
Sampling Method
Due to limited resources, there is almost always the need to sample respondents for any investigation (Saunders et al 2007). In this study, the researchers used simple random sampling. Simple random sampling is a type of probability sampling wherein every member of the population has an equal chance of being selected. The respondents in this study will be limited to employed Filipino nurses in hospitals of Negros Occidental and Iloilo as there are certain limitations. The sample size will be 50 respondents for this study.
Data Collection Method
For purposes of this research, primary data was collected through the employment of questionnaires. Correspondingly, primary data is an information collected through original or first hand research. A questionnaire is a set of printed or written questions with a choice of answers, devised for the purposes of a survey or statistical study. It is commonly used to understand the general characteristics or opinions of a group of people by distributing it to a sample online and in person.
Data Analysis Method
The data analysis of this research will be mostly presented in a qualitative manner. Descriptive analysis was used to analyze the data gathered from the respondents. Descriptive analysis is a summary statistic that quantitatively describes or summarizes features from a collection of information. It can provide an in-depth view of any topic that the researchers might want to study, and the level of detail that they can find in descriptive research is extremely valuable. However, this type of data analysis is only limited to a description of the occurrence in a population and it cannot test or verify the research problem statistically.
DISCUSSION:
This chapter presents the data gathered by the researchers that were summarized using different tables and graphs with their associated interpretations. Each graph shows the results of the survey conducted through an online survey platform that was answered by Filipino nurses that are employed in the Philippines. This chapter also presents the correlation analysis of the working conditions of overworked and underpaid nurses in the Philippines regarding their salary, workload, and discrimination.
Graph 1 shows that the pre-COVID pandemic salary range of 10,000-19,000 has the highest percentage of 54.9 percent. On the other hand, 23.5 percent of the respondents have the pre-covid salary range of 20,000-29,999, and 13.7 percent of the respondents range from 0-9,999 while the salary range of 30,000-39,999 has the lowest percentage of 7.8 percent.
Graph 1.

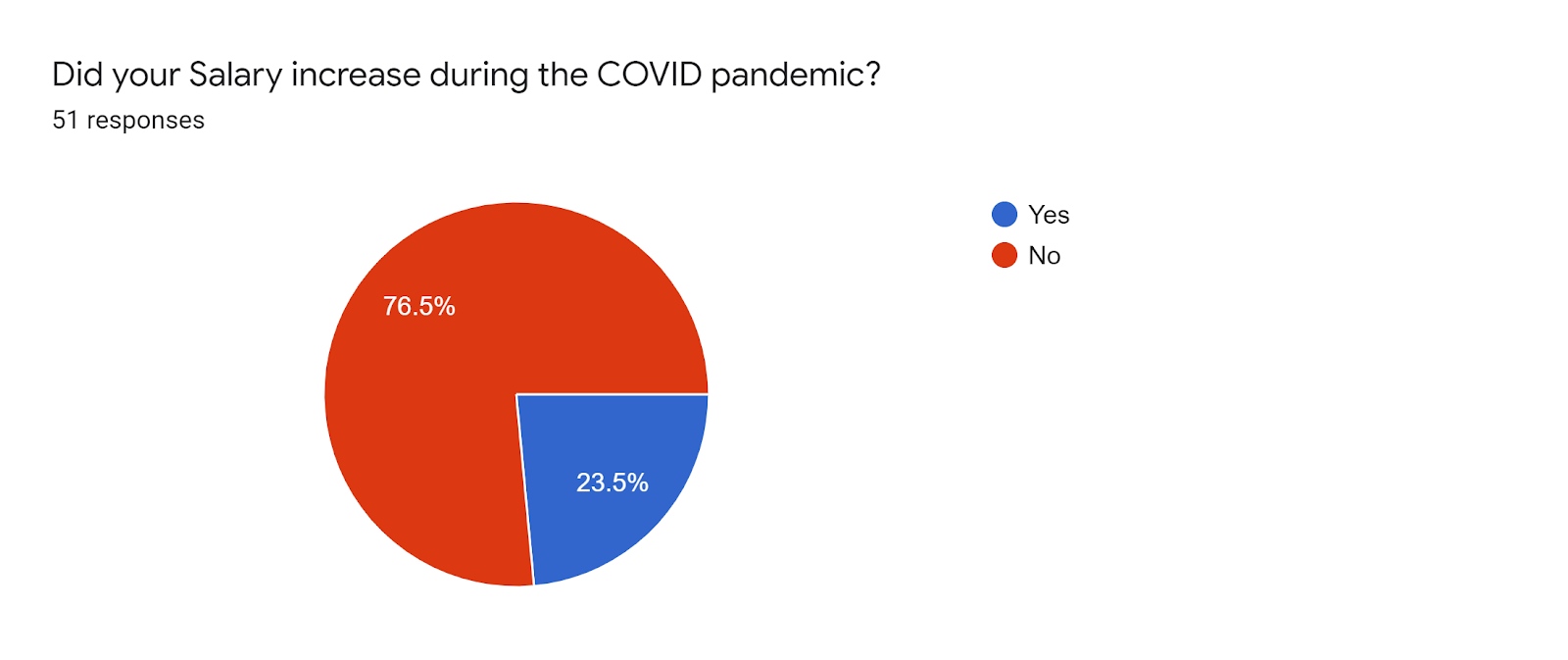
Graph 2 shows that 76.5 percent of the respondents indicated “No” that their salary did not increase during the COVID pandemic. On the other hand, only 23.5 percent of the respondents said “Yes”.
Graph 2
Graph 3 shows that 65 percent of the respondents have the highest salary range increase of 10,000-19,999 during the COVID pandemic. On the other hand, 20 percent of the respondents have the salary range increase of 20,000-29,999 while the salary range increase of 30,000-39,999 has the lowest percentage of 15 percent.
Graph 3

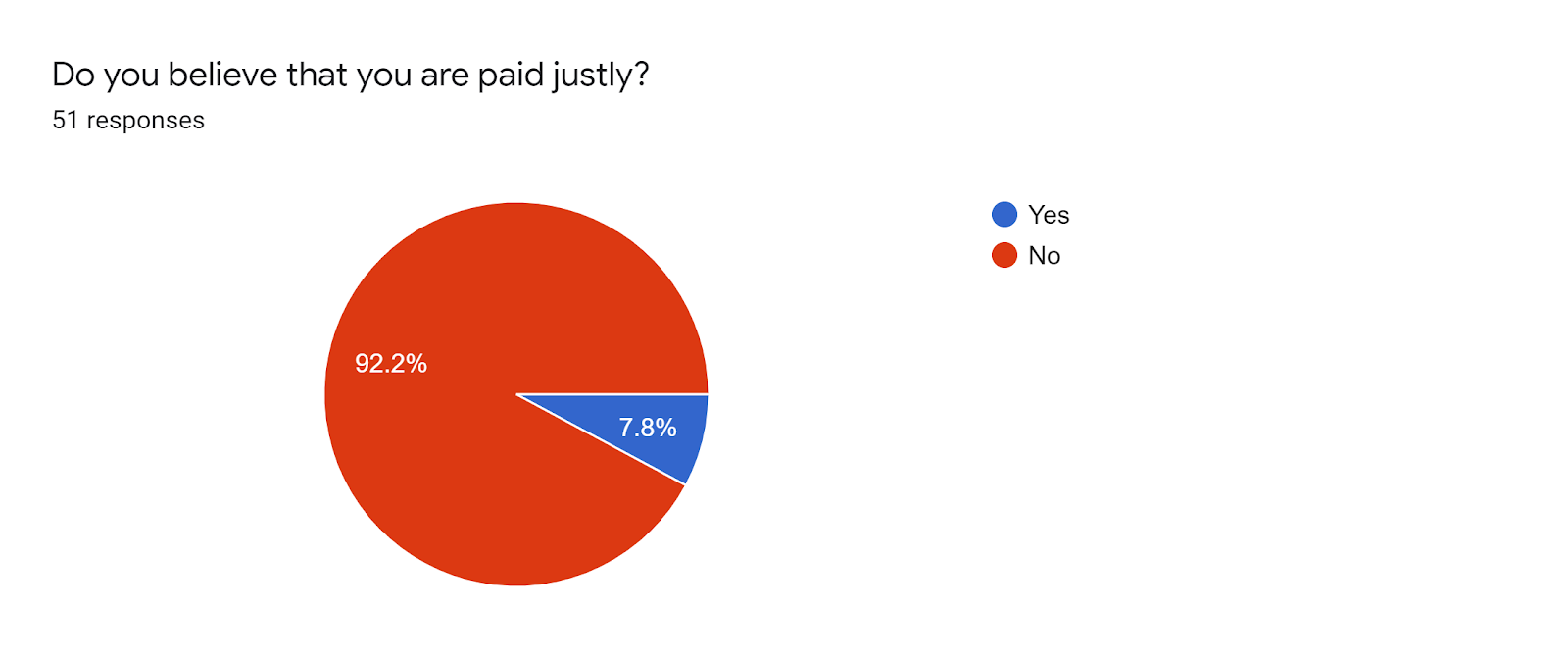
Graph 4 shows that 92.2 percent of the respondents answered “No” that they are not paid justly. On the other hand, 7.8 percent of the respondents answered “Yes”.
Graph 4
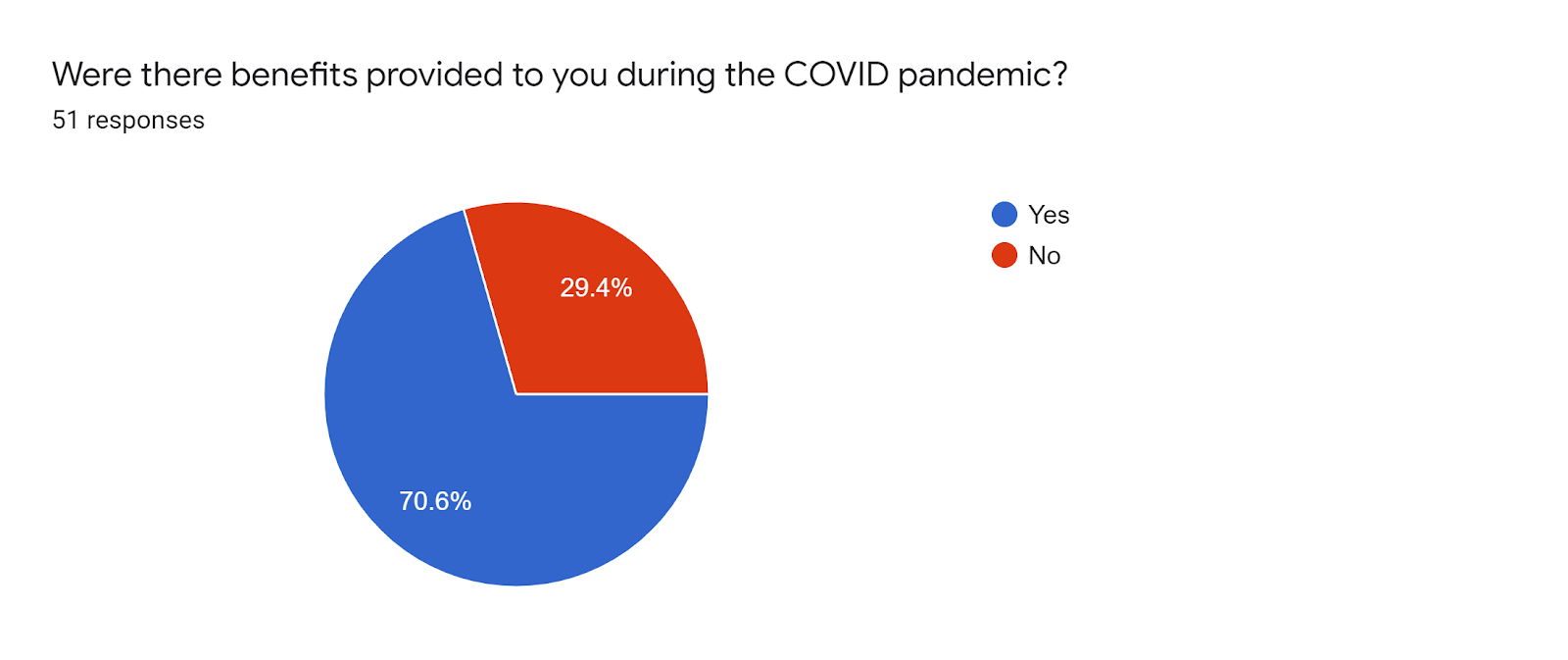
Graph 5 shows that 70.6 percent of the respondents answered “Yes” that they were benefits provided during the COVID pandemic. On the other hand, only 29.4 answered “No”.
Graph 5.
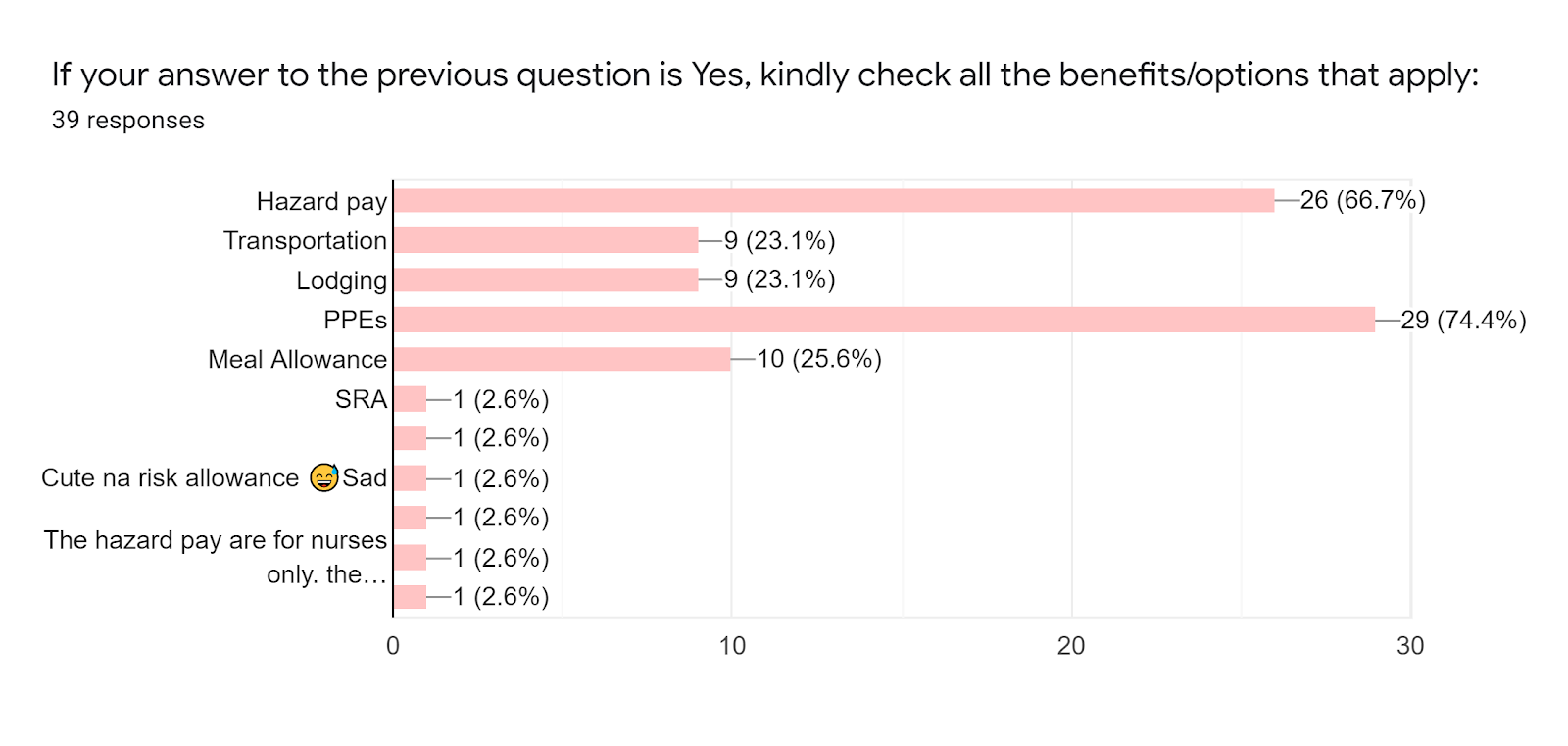
Graph 6 shows that 74.4 percent indicated that PPE’s was one of the benefits that was provided to the respondents. 66.7 percent answered hazard pay and only 23.1 percent answered transportation and lodging.
Graph 6.
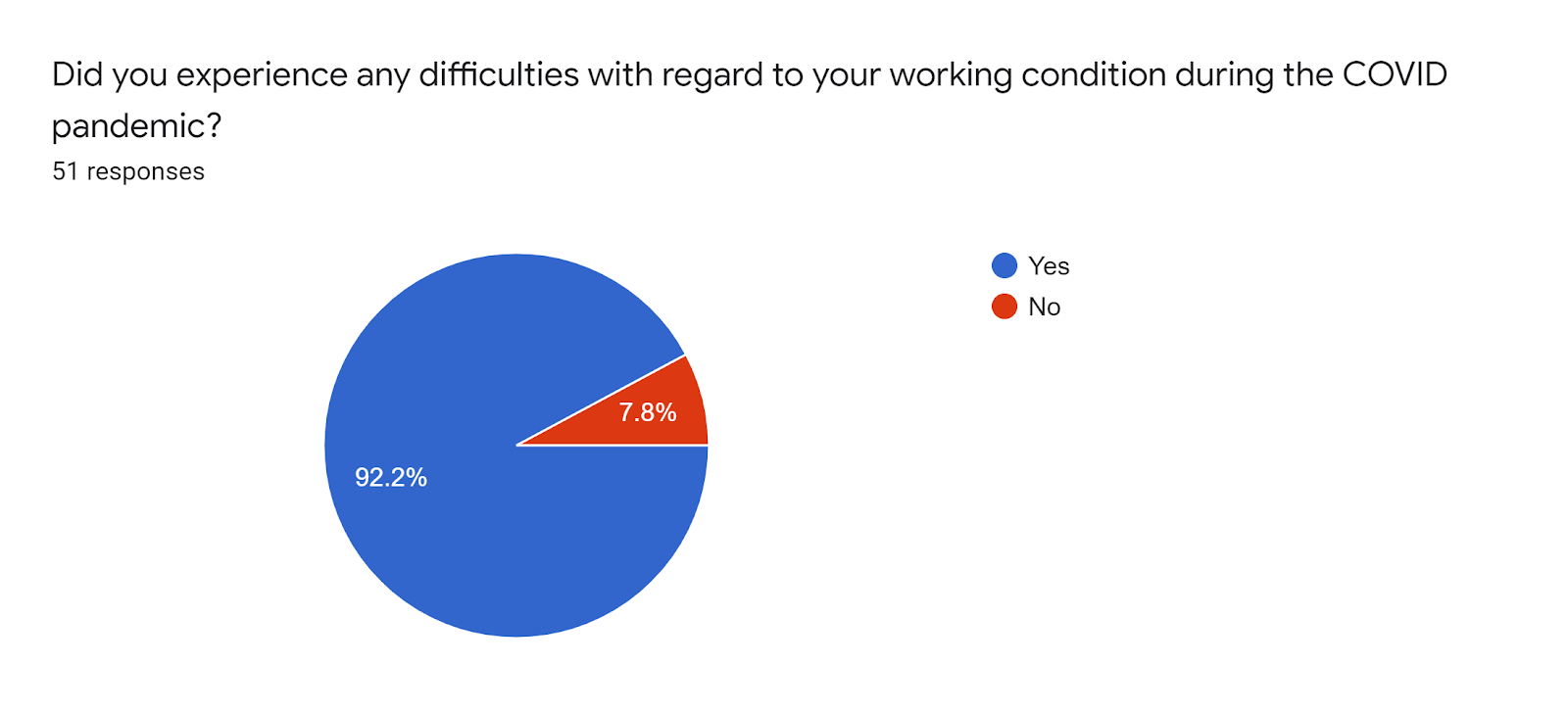
Graph 7 shows that 92.2 percent of the respondents indicated yes that they experienced difficulties regarding the working conditions during the COVID pandemic. On the other hand, only 7.8 percent said no.
Graph 7.
Graph 8 shows that 80.9 percent of the respondents who answered “Yes” under graph 7, indicated understaffing as one of the difficulties the respondents experienced in their workplace. 72.3 percent of the respondents indicated increased workload, 55.3 percent indicated increased work hours and only 4.3 percent experienced difficulties in transportation. Meanwhile, only 2.1 percent of the respondents indicated that the threat of infecting covid, using a low-level PPE, and that they are unsure of the truth of the patients they encounter whether or not the patients they encounter is infected with the virus as the difficulties they face in their workplace.
Graph 8.

Graph 9 shows that 77.6 percent of the respondents answered “Yes” that there were preventive measures exercised by their employer. On the other hand, only 22.4 percent of the respondents answered “No”.
Graph 9.

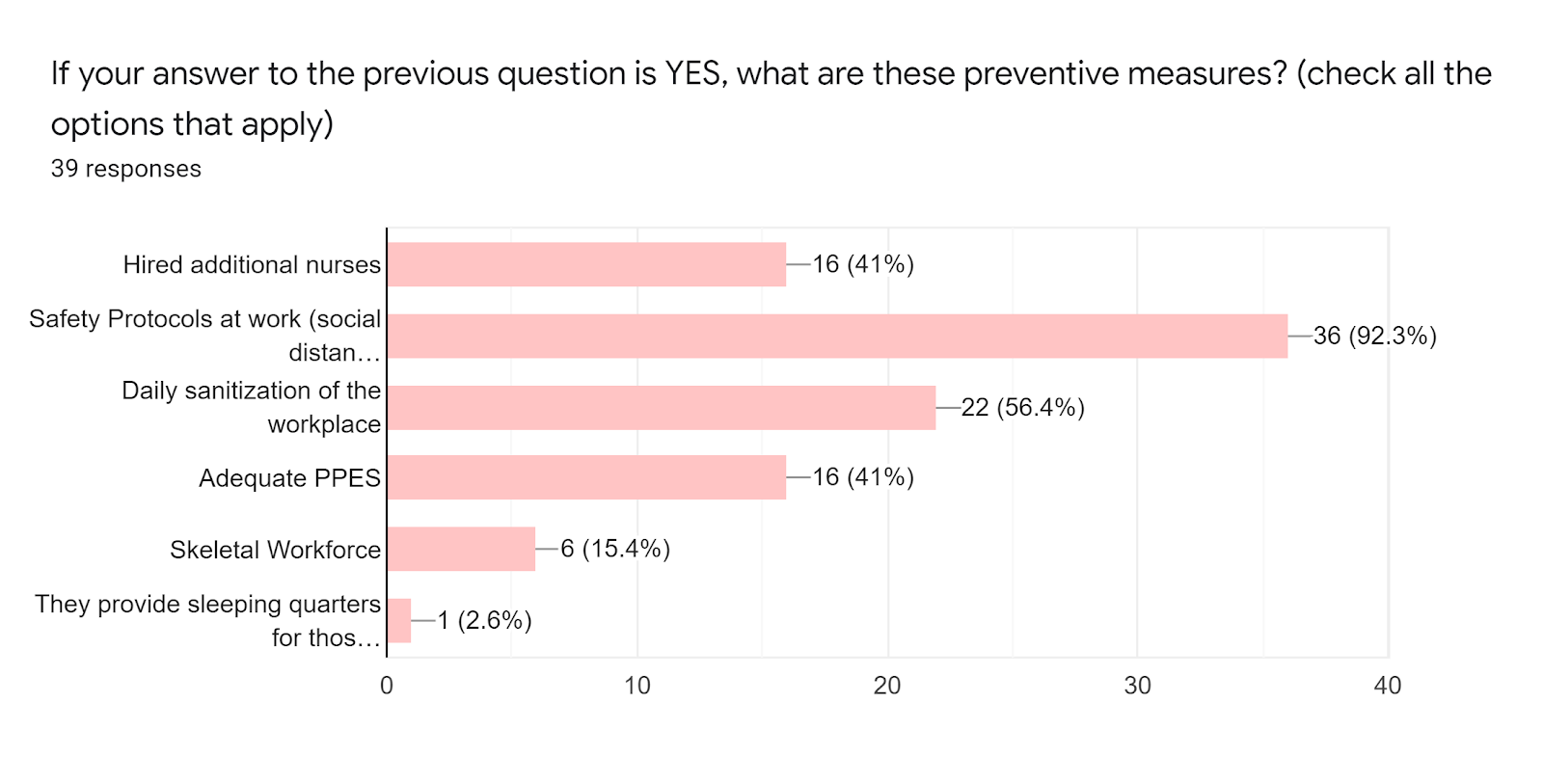
Graph 10 shows those who answered “Yes” in Graph 9 and that it indicates that 92.3 percent of the respondents indicated that safety protocols at work as one of the preventive measures. 56.4 percent indicated that there was daily sanitation of the workplace. 41 percent were the hiring of additional nurses and adequate PPE were given. 15.4 percent indicated that skeletal workforce as a preventive measure. Lastly, only 2.6 percent of the respondents indicated that they provide sleeping quarters to their staff.
Graph 10.
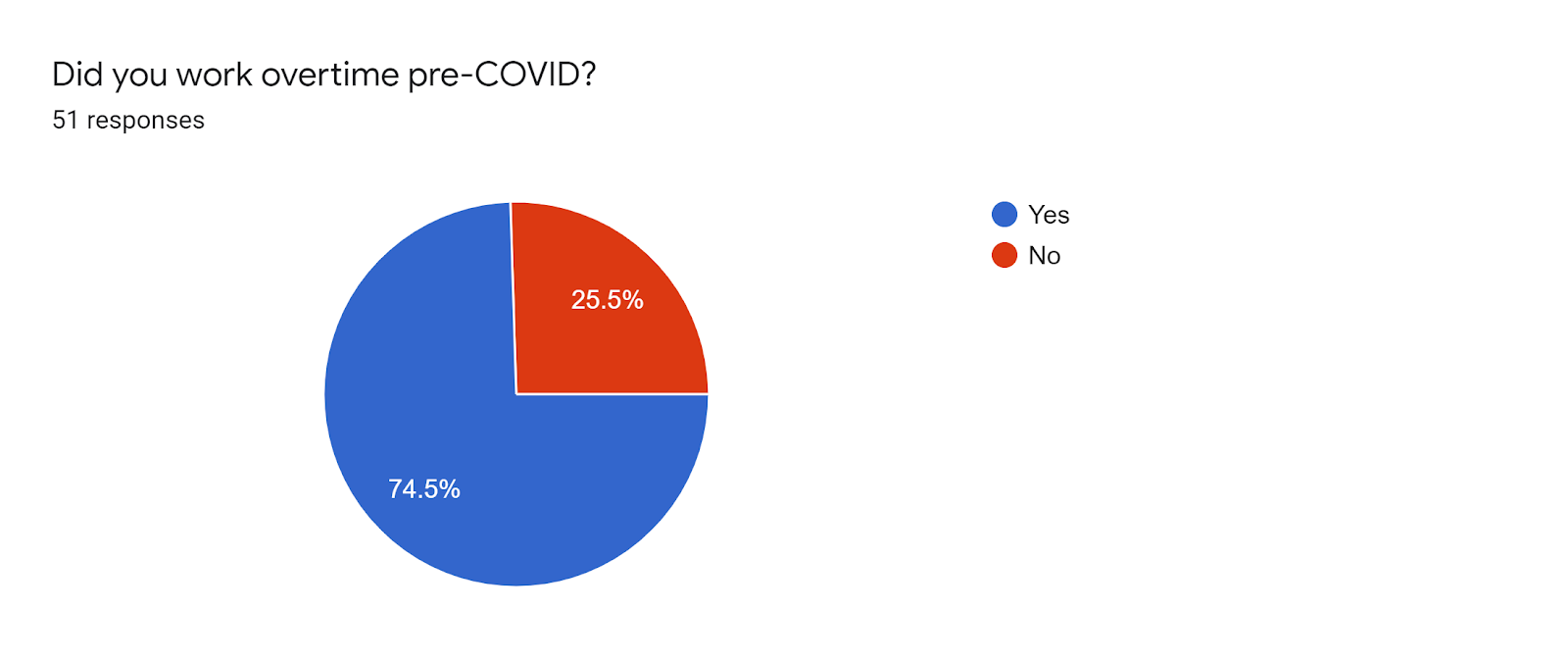
Graph 11 shows that 74.5 percent of the respondents answered “Yes” that they worked overtime pre-COVID. On the other hand, only 25.6 percent said “No”.
Graph 11.
Graph 12 shows that 21.6 percent of the respondents answered 2 to 3 hours as the average number of hours that they worked overtime pre-COVID. 18.9 percent of the respondents indicated that they worked overtime pre-COVID for 4 hours and more than 5 hours. On the other hand, only 13.5 percent answered that they worked overtime pre-COVID for only 1 hour.
Graph 12.

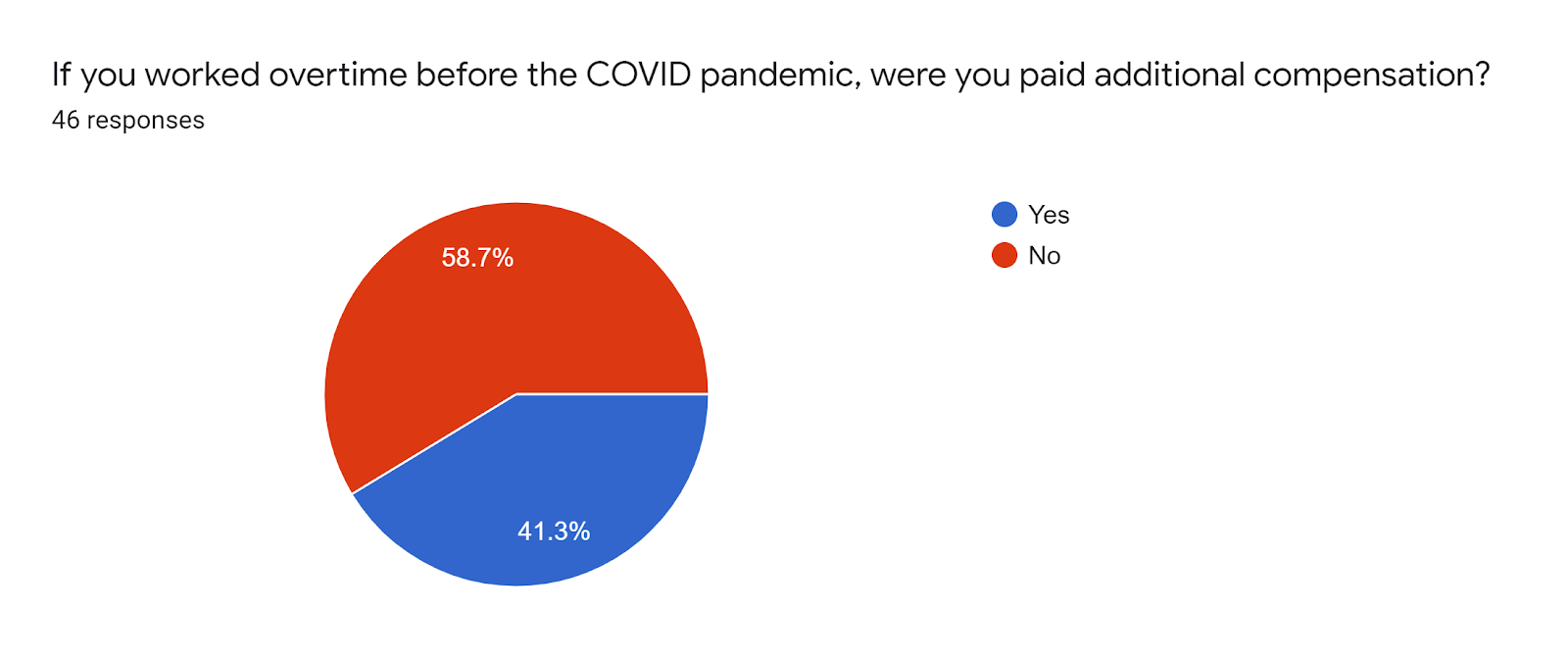
Graph 13 shows that 58.7 percent of the respondents answered “No” that they worked overtime before the COVID pandemic and were additionally compensated. On the other hand, only 41.3 percent answered “Yes”.
Graph 13.
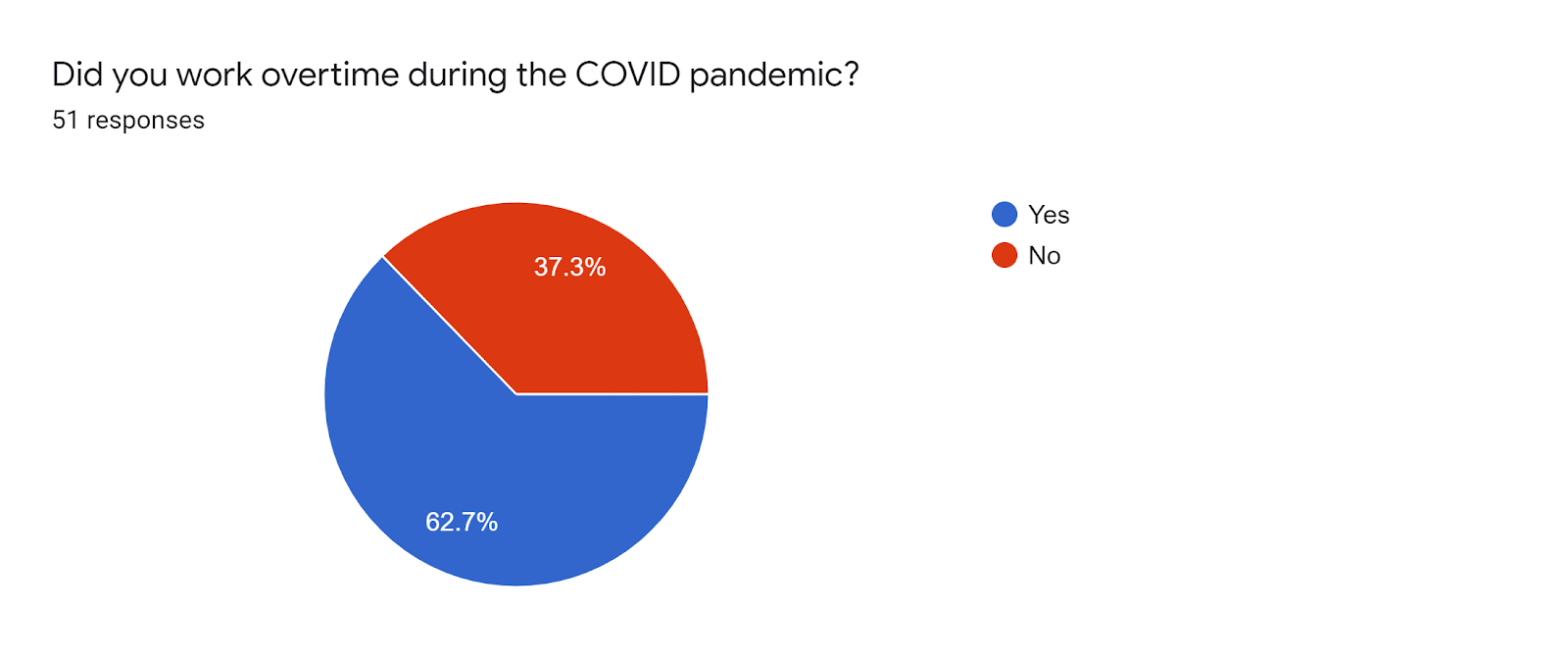
Graph 14 shows that 62.7 percent of the respondents answered “Yes” that they work overtime during the COVID pandemic. On the other hand, only 37.3 percent of the respondents answered “No”.
Graph 14.
Graph 15 shows that 27.3 percent of the respondents answered 2 hours as the number of hours they worked overtime during the COVID pandemic. 18.2 percent of the respondents answered that they worked overtime for 3 hours and more than 5 hours. 15.2 percent answered that they worked overtime during the COVID pandemic for 4 hours. Lastly, only 9.1 percent answered that the daily average number of hours that they worked overtime is 1 hour.
Graph 15.

Graph 16 shows that 52.5 percent of the respondents answered “No” that they were additionally compensated for their overtime during the COVID pandemic. On the other hand, only 47.5 percent answered “Yes” that they were paid additional compensation for their overtime during the COVID pandemic.
Graph 16.

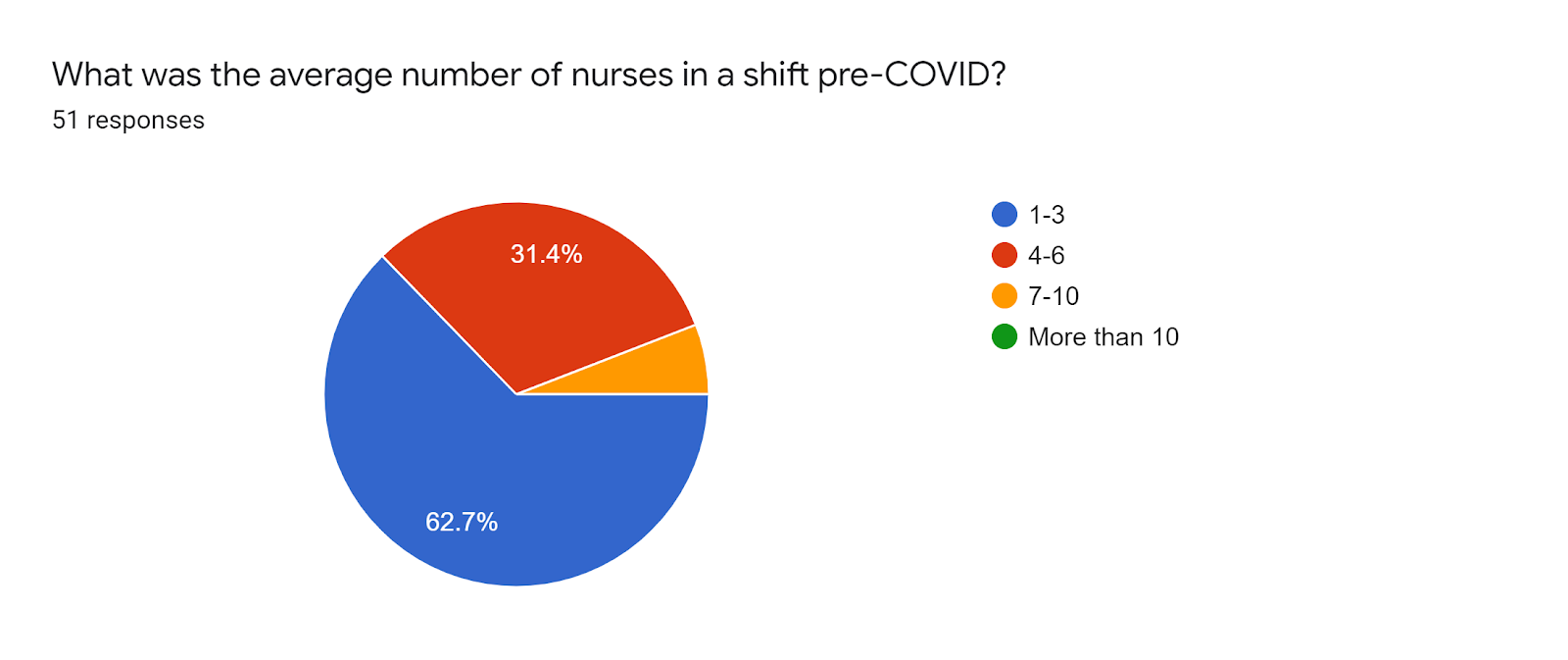
Graph 17 shows that 62.7 percent of the respondents indicated that the average number of nurses in a shift pre-COVID is 1 to 3. On the other hand, only 31.4 percent of the respondents indicated 4 to 6.
Graph 17.
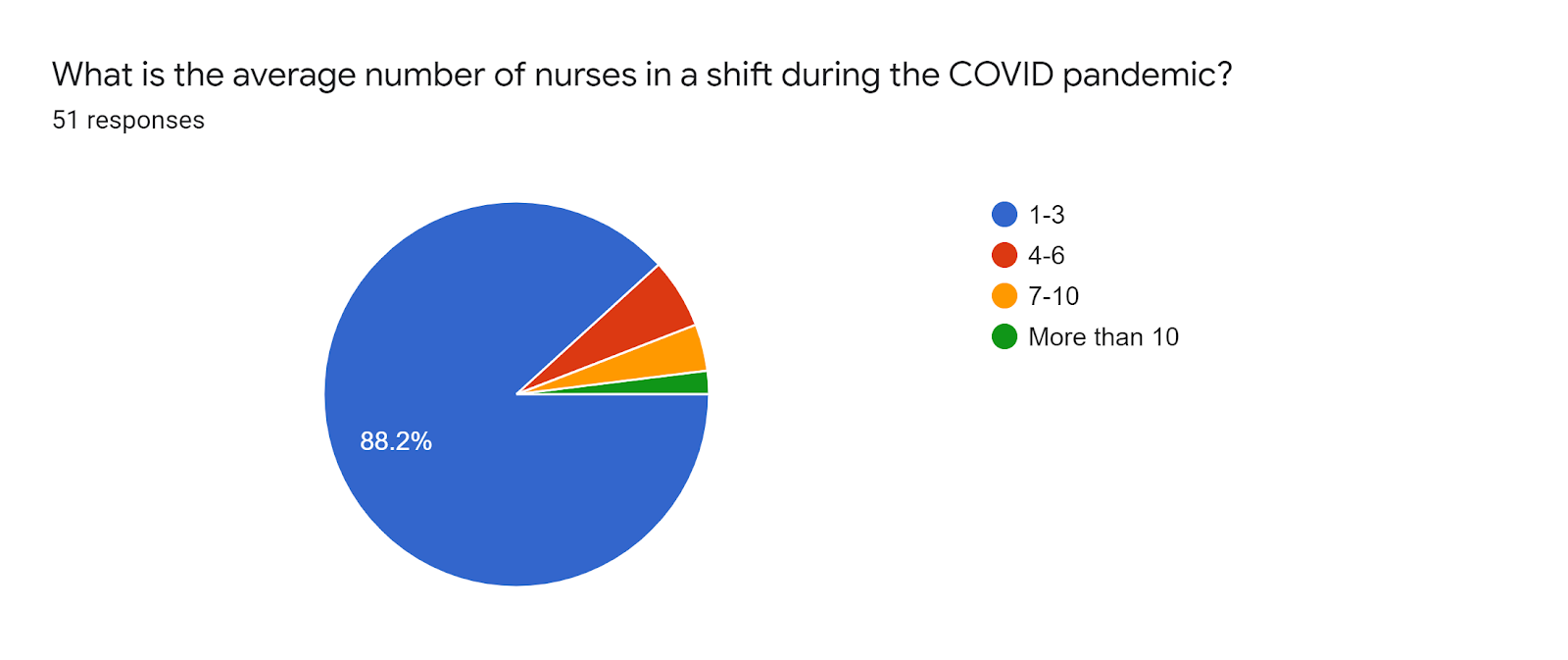
Graph 18 shows that 88.2 percent of the respondents indicated that the average number of nurses in a shift during the COVID pandemic is only 1 to 3. On the other hand, the minority of the respondents indicated more than 3.
Graph 18.
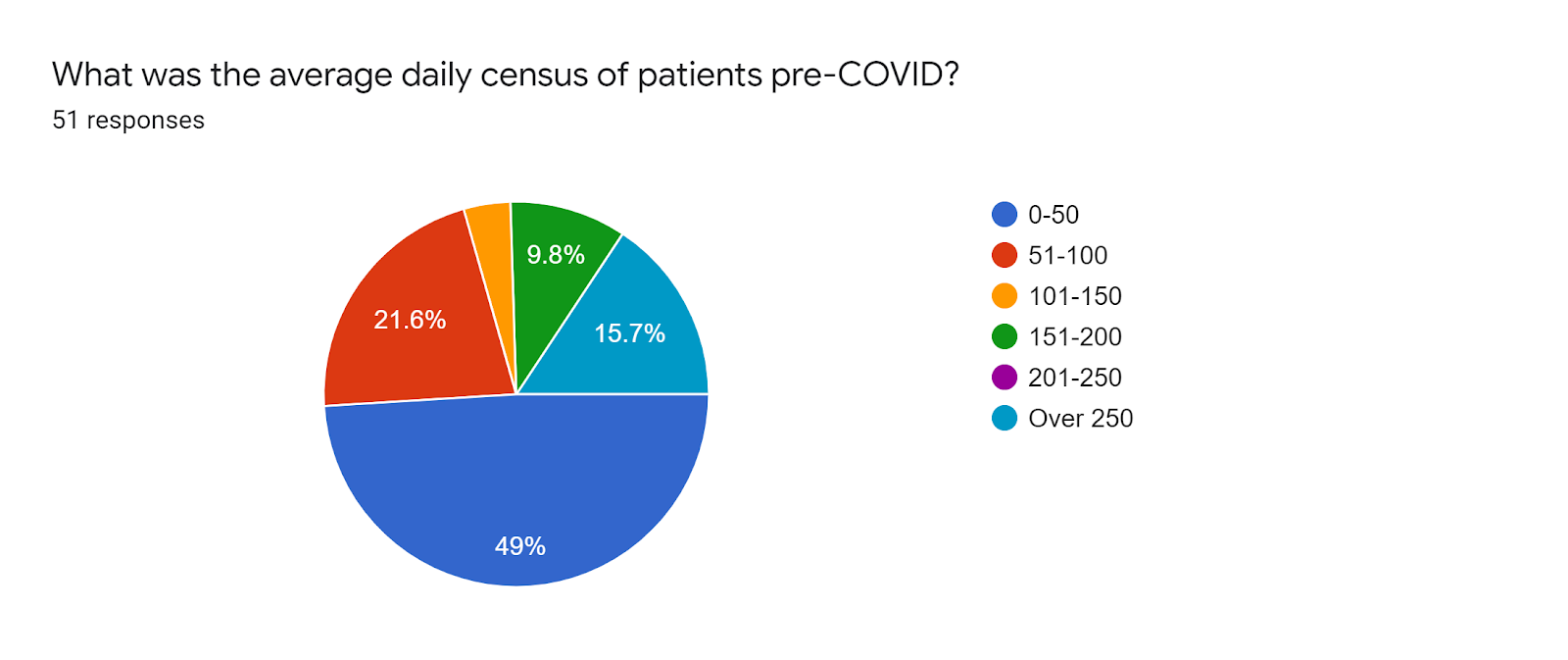
Graph 19 shows that 49 percent of the respondents indicated that the average daily census of patients pre-COVID is 0 to 50. 21.6 percent of the respondents indicated 51-100. 15.7 of the respondents indicated that the daily census of patients pre-COVID is over 250. Lastly, only 9.8 percent of the respondents that the average daily census of patients pre-COVID is 151 to 200.
Graph 19.
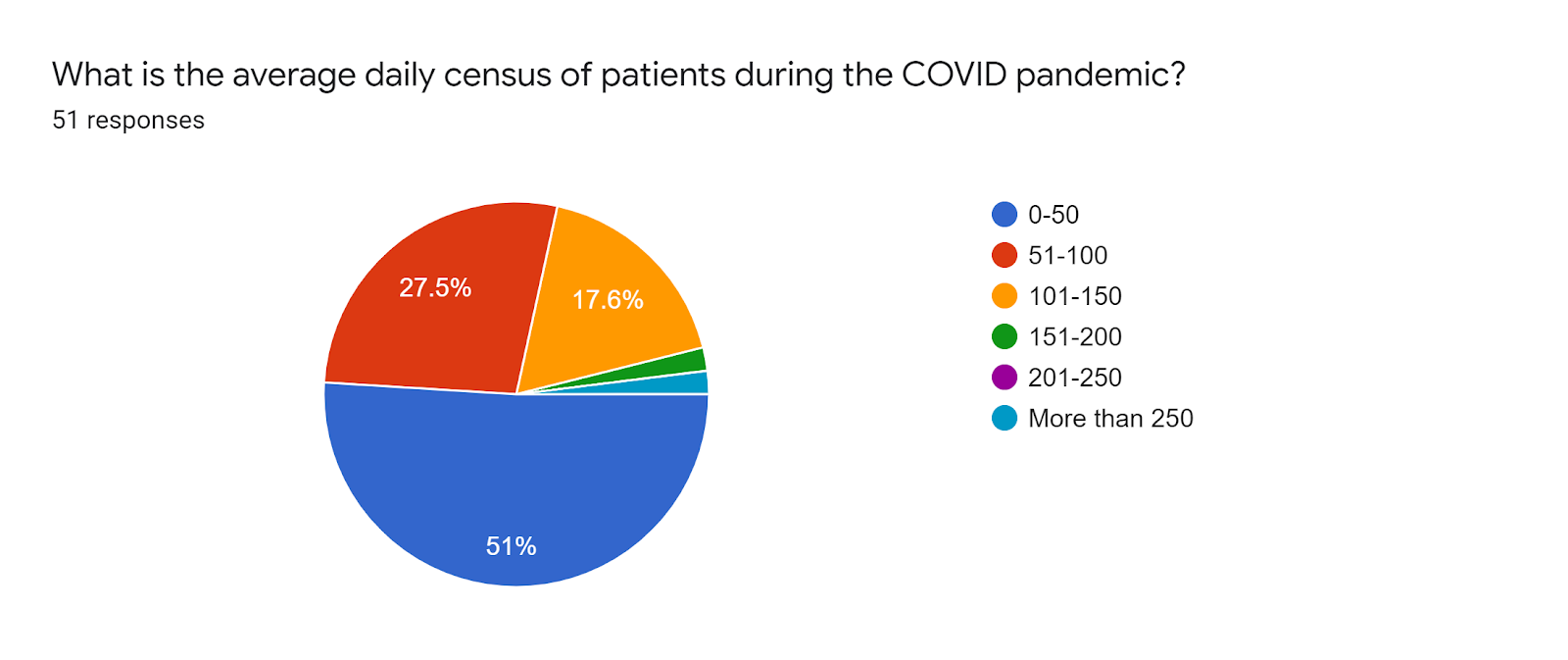
Graph 20 shows that 51 percent of the respondents indicated that the average daily census of patients during the COVID pandemic is 0 to 50. 27.5 percent of the respondents indicated 51 to 100. On the other hand, onty 17.6 percent of the respondents indicated that the average daily census of patients during the COVID pandemic is 101 to 150.
Graph 20.
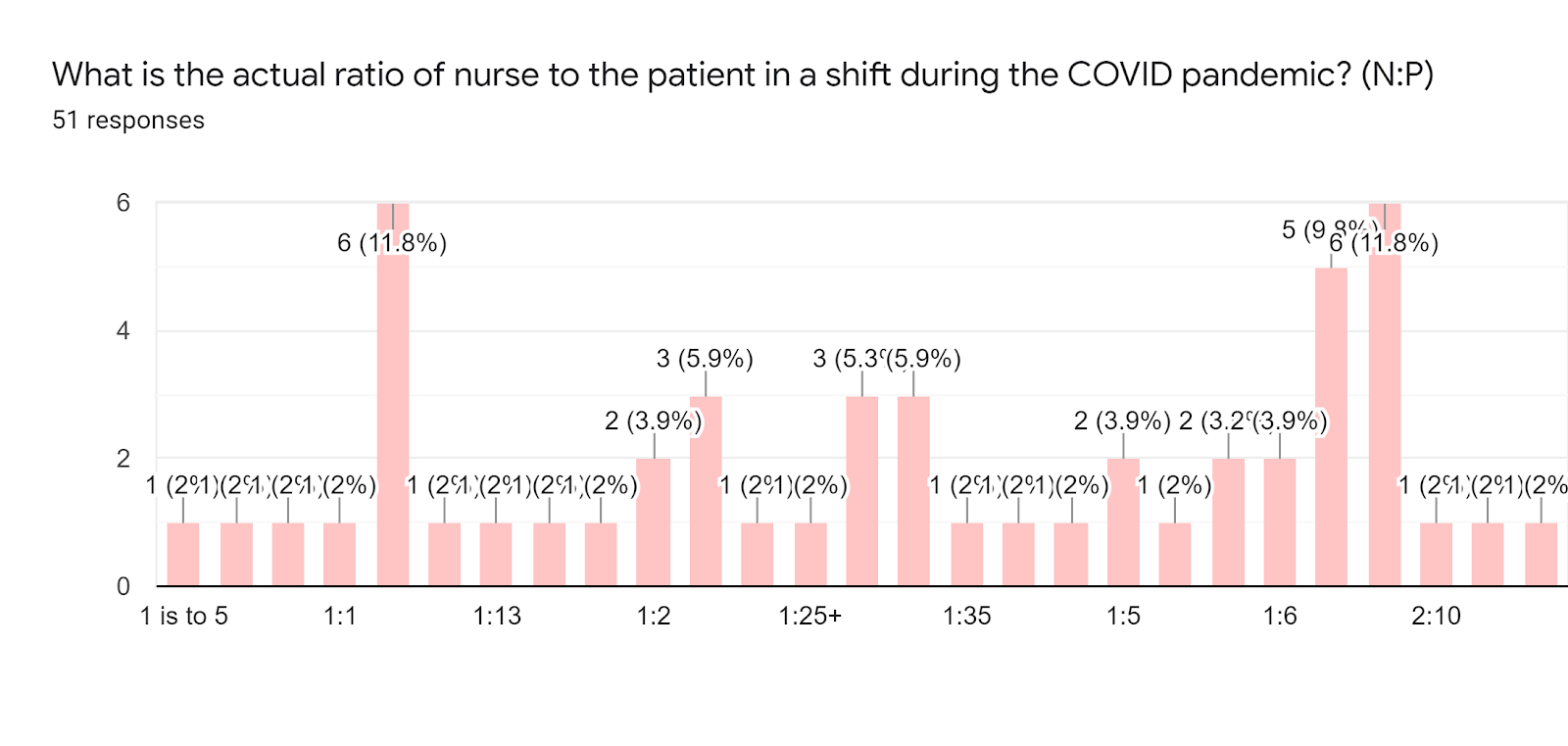
Graph 21 shows that 9.8 percent of the respondents indicated that the actual ratio of nurse to patient in a shift pre-COVID is “1:10”.

Graph 22
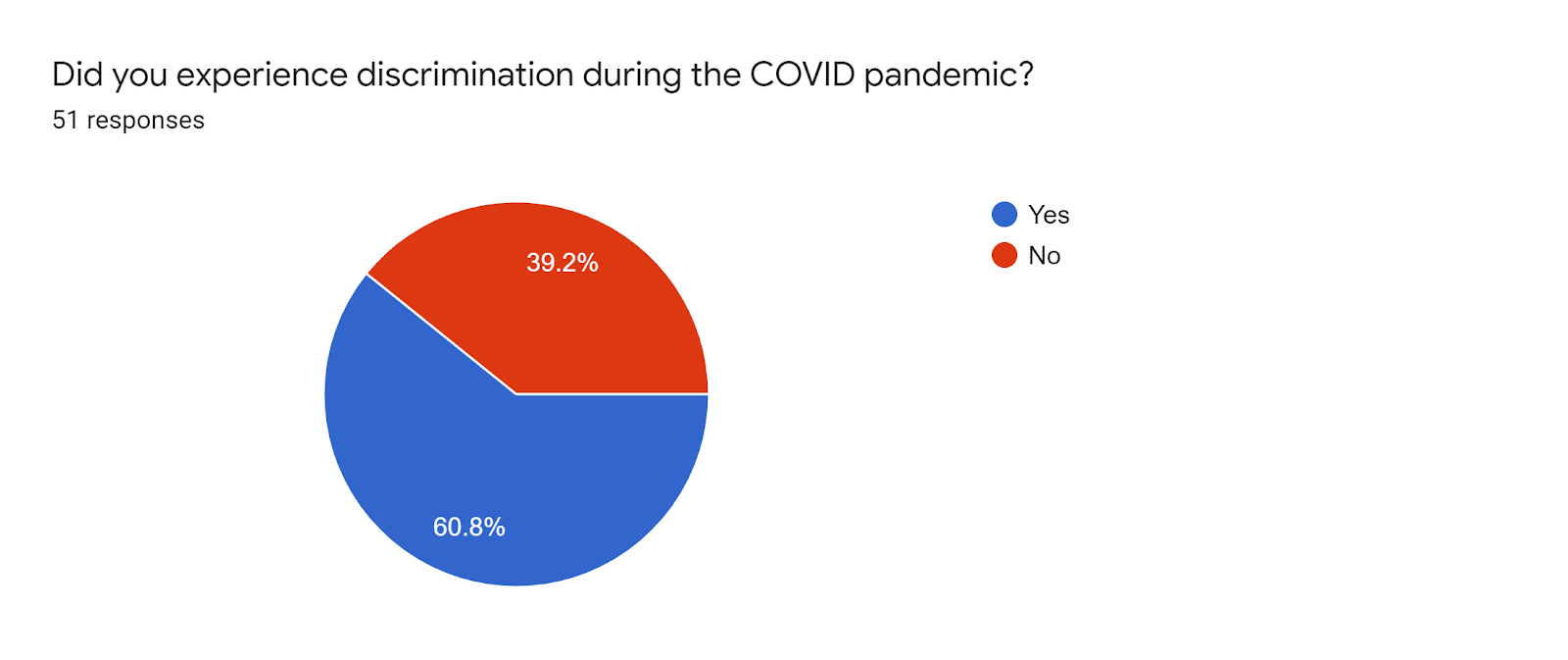
Graph 23 shows that 60.8 percent of the respondents answered “Yes” that they experience discrimination during the COVID pandemic. On the other hand, only 39.2 percent answered “No”.
Graph 23.
CONCLUSION:
Based on the findings of the study, the following conclusions were derived:
The study has shown that the average salary range of Philippine nurses pre-COVID pandemic is 10,000 to 19,999 pesos. Moreover, the majority of the respondents answered that their salary did not increase during the COVID pandemic. The minority of the respondents answered that their salary did increase during the COVID pandemic, however, the salary increase was still in the average range of 10,000 to 19,000 pesos. Most of the respondents indicated that they experienced difficulties during the COVID pandemic and the majority of these difficulties they experience in their workplace are mostly understaffing, increased workload, and the increase in their working hours. As for the difficulties, the respondents’ experience in their workplace is concerned, most of the respondents also worked overtime during the COVID pandemic and the majority of the respondents with regards to their overtime were not paid additional compensation. Lastly, the majority of the respondents experience discrimination in their line of work, and most of this discrimination occurred in public places and also
RECOMMENDATION:
The researchers identified a range of areas for attention in relation to The Working Conditions of Overworked and Underpaid Nurses in the Philippines during a Pandemic , which are provided in the other parts of this paper. The following recommendations for research are based on the study findings:
- Our research data showed that 76.5% of our respondents claim that their salary did not increase during the COVID pandemic and 92.2% said that they are not paid justly as nurses, while facing difficulties in the workplace such as Understaffing, Increased workload, and increased work hours, among many others. This is likely due to the large demand in the workforce, but not enough workers in the workplace. Further research is recommended to determine tangible and intangible solutions to the problem.
- For future research, include other variables such as scope, geographical location, economic status, and other factors that may affect the compensation and working conditions of nurses.
- Do not limit gathering data from 1-5 hospitals only. Gather information from across a certain area to get more diverse inputs and responses.
- In addition, this report recommends further work to: ·
- make an assessment of the demand of nurses in our country;
- quantify the exact ratio of nurse to the patient in a shift;
- establish the proper salary rates that can compete with international rates for our nurses;
- research further on specific solutions to better compensate the overworked nurses in our country
